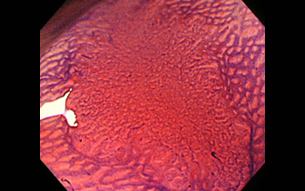
Depressed type of colorectal cancer
Colorectal cancer development and progression
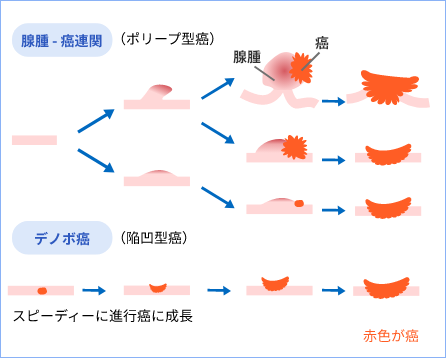
There are two main routes by which colorectal cancer develops.
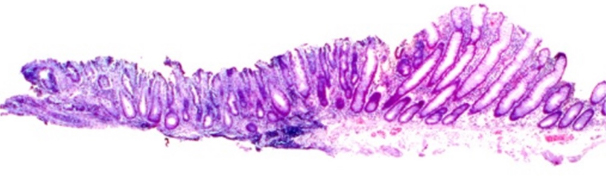
There are two pathways: benign adenomas (polyps) that grow slowly into advanced cancer, and there is de novo carcinoma, which appears with cancerous cells from the first development. This has a rapid growing depressed type of cancer that differs from polyp type cancer.
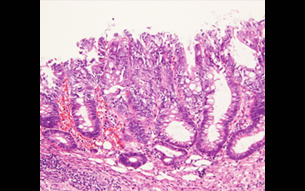
This depressed type of cancer is a difficult to detect and can metastasise even at a stage as small as 10 mm or less.
History of depressed type colorectal cancer (IIc)
Before the 1980s, colorectal cancer was thought to arise from polyps.
The flat and depressed type of cancer is difficult to detect and is not detected, so it did not exist and was referred to as a ‘phantom cancer’.
In the 1985s, Dr Shin'ei Kudo of Akita Red Cross Hospital had been found many depressed-type cancers and proved that they existed, but there were no doctors other than Dr Kudo who could find out depressed-type cancers, and the academic community made fun of the idea that it was an ‘endemic disease in Akita’.
The director wanted to learn more about colonoscopy, so he trained for two years from 1990 at Akita Red Cross Hospital under Dr Shin'ei Kudo, where he learnt a lot, including the detection of depressed-type cancers.
In 1995, when I visited from the National Cancer Centre East Hospital to the University of Leeds in the UK to teach colonoscopy as part of a joint UK-Japan research project, the director detected two cases of depressed-type cancer in the UK, which had only been found in Japan. This achievement has helped to prove that depressed-type cancer is a global disease.
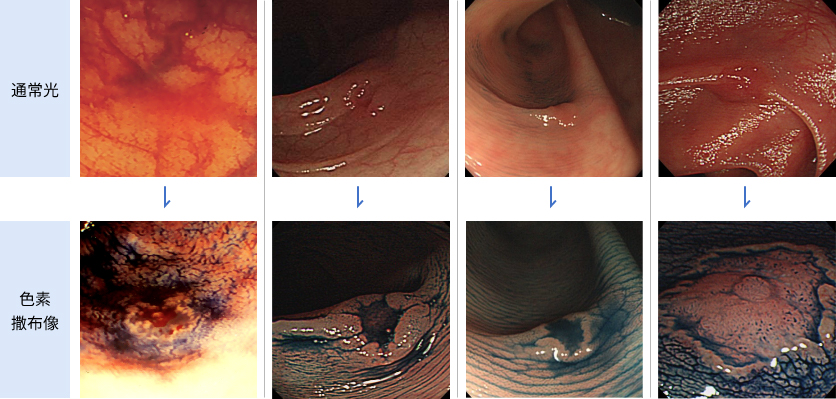
How to detect depressed-type cancer (IIc) endoscopically.
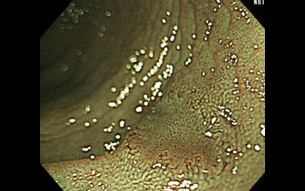
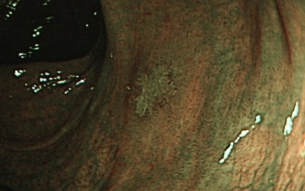
Until around 2008, the redness of the mucosa was detected by white light (top photo).
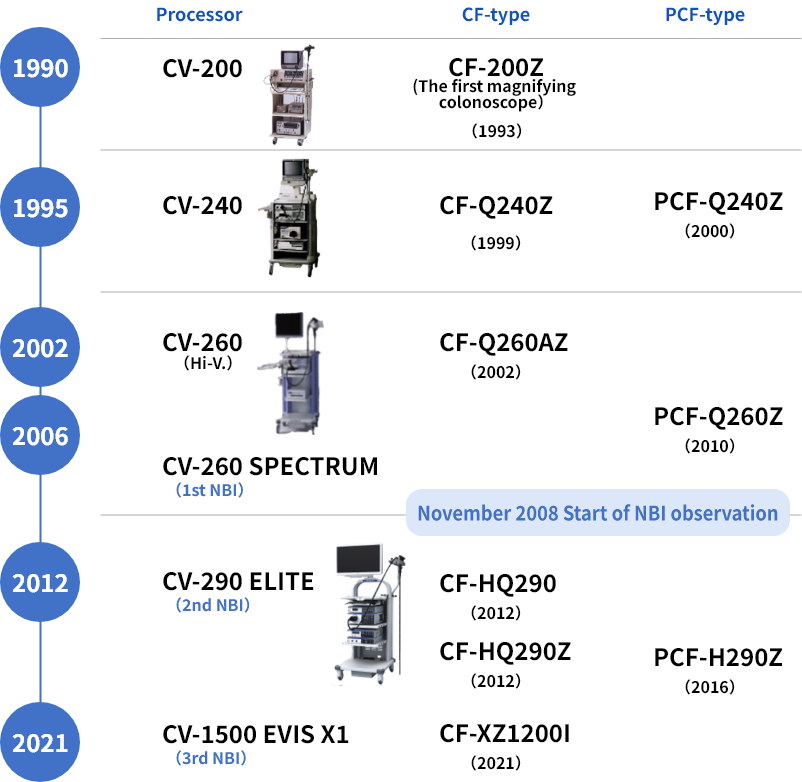
Historical evolution of colonoscope models.
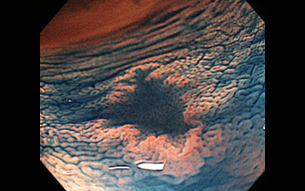
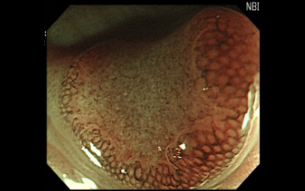
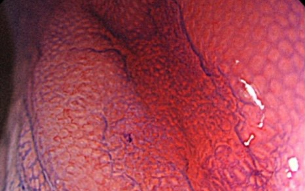
O-ring sign This O-ring sign is a finding to detect IIc by NBI observation (Director's suggestion).
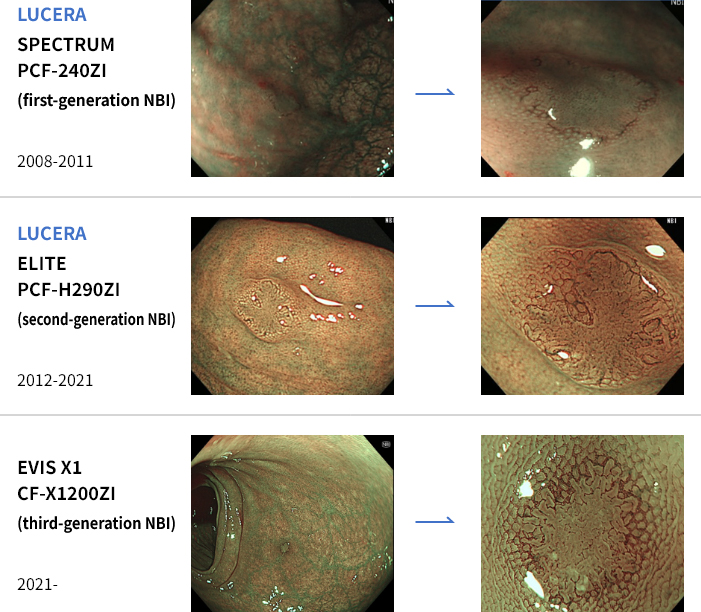
Endoscopic equipment has evolved and the first generation of NBI in the upper photo shows insufficient light intensity.
The lack of light intensity has been resolved in the second and third generation NBI, especially the latest CF-X1200ZI, which is brighter and has clearer image quality, and O-ring signs can be seen clearly from a distance, making it useful for the detection of depressed-type tumor.
2017 Presentation of IIc detection by NBI at the United of European Gastroenterology (UEGW: Barcelona).
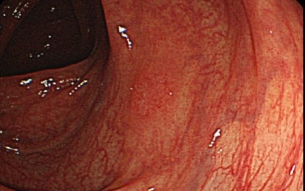
Since 2008, NBI observations have been used to detect IIc.
With advances in endoscopic equipment, the light intensity and image quality of NBI has evolved, and from the second generation of NBI, the detection of IIc has become easier.
IIc found by NBI, the depression margins appear as brown rings. The Director proposed this as an O-ring sign as a finding of IIc and presented it in Barcelona in 2017.
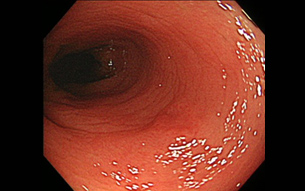
4●, male, 6 mm,
IIc (detected by first-generation NBI).



4●, male, 5 mm,
IIc (detected by first-generation NBI)



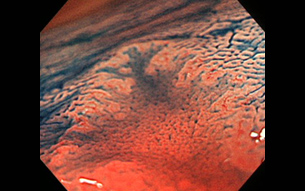
5●, male,
IIc detection by second-generation NBI.